
Scientific Calendar August 2019
How can the immature platelet fraction (IPF) help in the differential diagnosis of thrombocytopenia?
Thrombocytopenia with a decreased IPF may indicate increased platelet destruction in peripheral blood.
Thrombocytopenia with an increased IPF may indicate decreased platelet production in bone marrow.
Thrombocytopenia with an increased IPF may indicate increased destruction in peripheral blood, loss of platelets or a hereditary macrothrombocytopenia.
Congratulations!
That's the correct answer!
Sorry! That´s not completely correct!
Please try again
Sorry! That's not the correct answer!
Please try again
Notice
Please select at least one answer
Graphics
References
[2] Van De Wyngaert Z et al. (2019) Immature platelet fraction (IPF): A reliable tool to predict peripheral thrombocytopenia. Curr Res Transl Med. 2019 Apr 12. pii: S2452-3186(19)30017-0. doi: 10.1016/j.retram.2019.04.002. [Epub ahead of print]
[3] Miyazaki K et al. (2015) Immature platelet fraction measurement is influenced by platelet size and is a useful parameter for discrimination of macrothrombocytopenia. Hematology. 20(10):587-92.
Scientific background information
Thrombocytopenia is a condition characterised by an abnormally low platelet count – lower than the normal platelet count in adults that ranges from 150 x 109/L to 450 x 109/L. Overlooking a severe thrombocytopenia can have serious consequences for the patient, so obtaining reliable platelet counts is essential for making clinically important decisions with confidence. Although thrombocytopenia is defined by low platelet concentrations, PLT counts alone do not reveal the underlying causes, which can be inherited or acquired. The causes can be divided into two main categories: decreased bone marrow production and increased destruction/consumption of platelets in peripheral blood. Often, the clinical question is whether thrombocytopenia is due to bone marrow failure as observed in conditions such as aplastic anaemia, myelodysplastic syndromes, and drug toxicity, or due to increased peripheral destruction/consumption such as in immune thrombocytopenia, thrombotic thrombocytopenic purpura or disseminated intravascular coagulation. Invasive bone marrow biopsies are usually recommended to investigate the underlying aetiology [1].
Differential diagnosis of thrombocytopenia is complex and requires an investigation of the patient’s medical history, an evaluation of clinical symptoms and an assessment of blood-derived platelet parameters. The immature platelet fraction (IPF) is a marker of platelet production and indicates the percentage of immature platelets in relation to the total PLT count. Several publications reported that IPF obtained from the Sysmex XE- and XN-Series analysers is higher in patients with thrombocytopenia caused by excessive platelet destruction/consumption than in patients with thrombocytopenia caused by decreased platelet production in bone marrow [1].
Recently, a study from Van De Wyngaert et al. investigated patients who underwent bone marrow aspiration to explore thrombocytopenia with the aim of establishing a cut-off value to distinguish a peripheral from a central mechanism of thrombocytopenia. In this multicentric study, an IPF higher than 13% was found to be predictive of peripheral thrombocytopenia, and this measurement could avoid bone marrow aspirations, especially when thrombocytopenia is the sole abnormality in the full blood count. With isolated thrombocytopenia, bone marrow aspiration could have been avoided in 66% of patients [2].
The IPF can also contribute to the differential diagnosis of suspected congenital thrombocytopenia. Congenital thrombocytopenia is usually suspected in the case of neonatal thrombocytopenia, the onset of bleeding symptoms in childhood, a family history of thrombocytopenia, or when the PLT count is unresponsive to ITP treatment. For example, Miyazaki et al. revealed how IPF can contribute to the differential diagnosis of congenital thrombocytopenia. A markedly elevated IPF suggests congenital macrothrombocytopenia [3].
Differential diagnosis of thrombocytopenia ‒ clinical cases
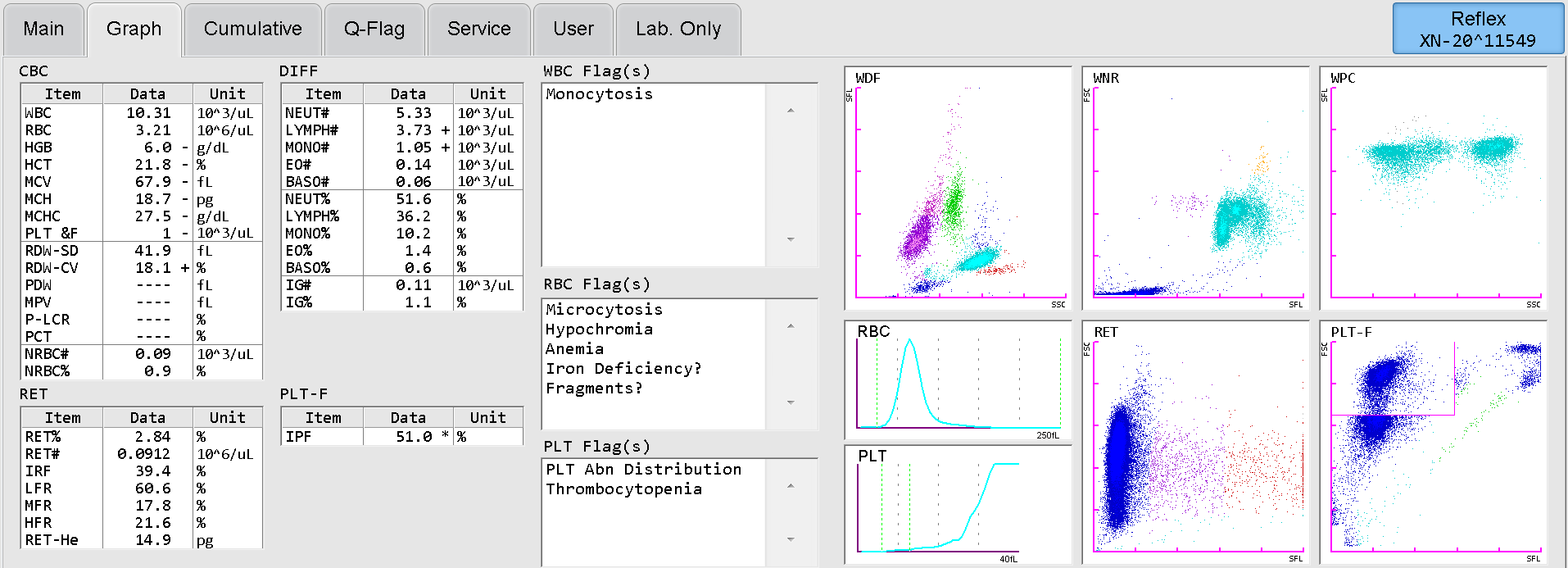
In a case of a 37-year-old female, who was admitted to hospital due to skin bleeding and strong menstruation, severe thrombocytopenia and anaemia was found on day 1 on the Sysmex automated haematology analyser XN-Series (Fig. 1) and, with the help of a highly increased IPF, immune thrombocytopenia was diagnosed. The patient was successfully treated with a high-dose corticosteroid pulse therapy followed by oral steroids for four months without platelet transfusion. Rapid and complete remission of the immune thrombocytopenia was achieved and the PLT count quickly normalised.
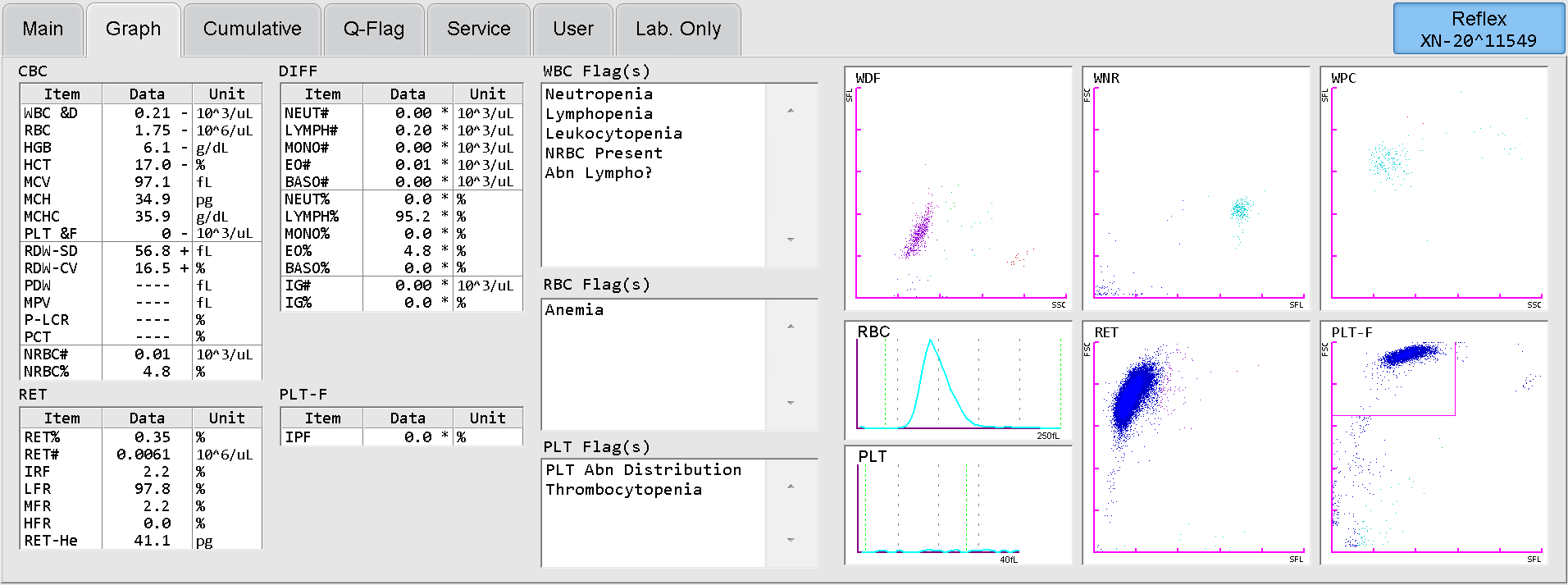
Another case is that of a 74-year-old female, who was admitted to hospital due to fever and massive skin and gastrointestinal bleeding. On the day of admission, severe pancytopenia and gram-negative sepsis was diagnosed and, with the aid of an IPF = 0 %, bone marrow failure was found (Fig. 2). The patient was successfully treated with antibiotics, corticosteroids, filgrastim, multiple erythrocyte and platelet transfusions and other supportive care. The complete bone marrow recovery was achieved after four weeks.
