
Scientific Calendar June 2020
Hypertensive nephropathy
Why is the Sysmex Meditape 11A used on the UC-3500 an ideal tool for screening for albuminuria?
Because of its limit of detection of 5.5 mg/L
Because it also delivers the glomerular filtration rate
It offers correct judgement by correlation with creatinine
Congratulations!
That's the correct answer!
Sorry! That´s not completely correct!
Please try again
Sorry! That's not the correct answer!
Please try again
Notice
Please select at least one answer
Scientific background
Chronic kidney disease (CKD) is defined as abnormalities of the kidney structure or function that have been present for more than three months. The classification of CKD is based on the estimated glomerular filtration rate (eGFR) and albuminuria [KDIGO]. CKD is part of a disease continuum with various factors promoting the progression from acute kidney injury (AKI) to chronic kidney disease and then to end-stage renal disease (ESRD).
Besides a variety of different conditions, such as persistent urinary obstructions, chronic infections of the lower urinary tract, interstitial nephritis and polycystic kidney disease, hypertension is the second leading cause of end-stage renal disease, following diabetes mellitus.
Hypertension can be both a cause and an effect of chronic kidney disease and contributes to its progression by affecting all renal compartments: blood vessels, glomeruli and the tubular interstitial space.
Chronic hypertension causes hypertensive nephropathy that manifests as hypertensive nephrosclerosis through deposition of hyaline (hyalinosis) in afferent arterioles, leading to minimal changes in intraglomerular haemodynamics. Ongoing hyalinosis, however, causes narrowing and structural changes of the aorta and arteries, reducing their elasticity and haemodynamics. These structural changes and the related mechanical stress translate into glomerular damage (hypertensive glomerulopathy), for example by a partial ischaemia, narrowing the glomerular tuft and reducing the glomerular filtration rate. Within the glomeruli, podocytes interact to form a size-selective filtration barrier, essential for glomerular filtration and production of urine. Hypertension causes injury of podocytes and their irreversible detachment from the glomerular basement membrane and break-down of the barrier, leading to proteinuria. Hypertension also causes a large spectrum of lesions in renal tubular epithelial cells (RTEC), finally leading to a loss of cells and the release of pro-inflammatory substances. Angiotensin II, a vasoconstricting agent of the renin-angiotensin-system that regulates the blood pressure, is a known promotor of inflammatory and oxidative stress through the induction of cytokines and chemokines. This interaction induces the transition of epithelial cells into mesenchymal cells by a loss of cell polarity and change in cell adhesion and leads to tubule-interstitial fibrosis and the progression of chronic kidney disease [SECCIA].
Laboratory results
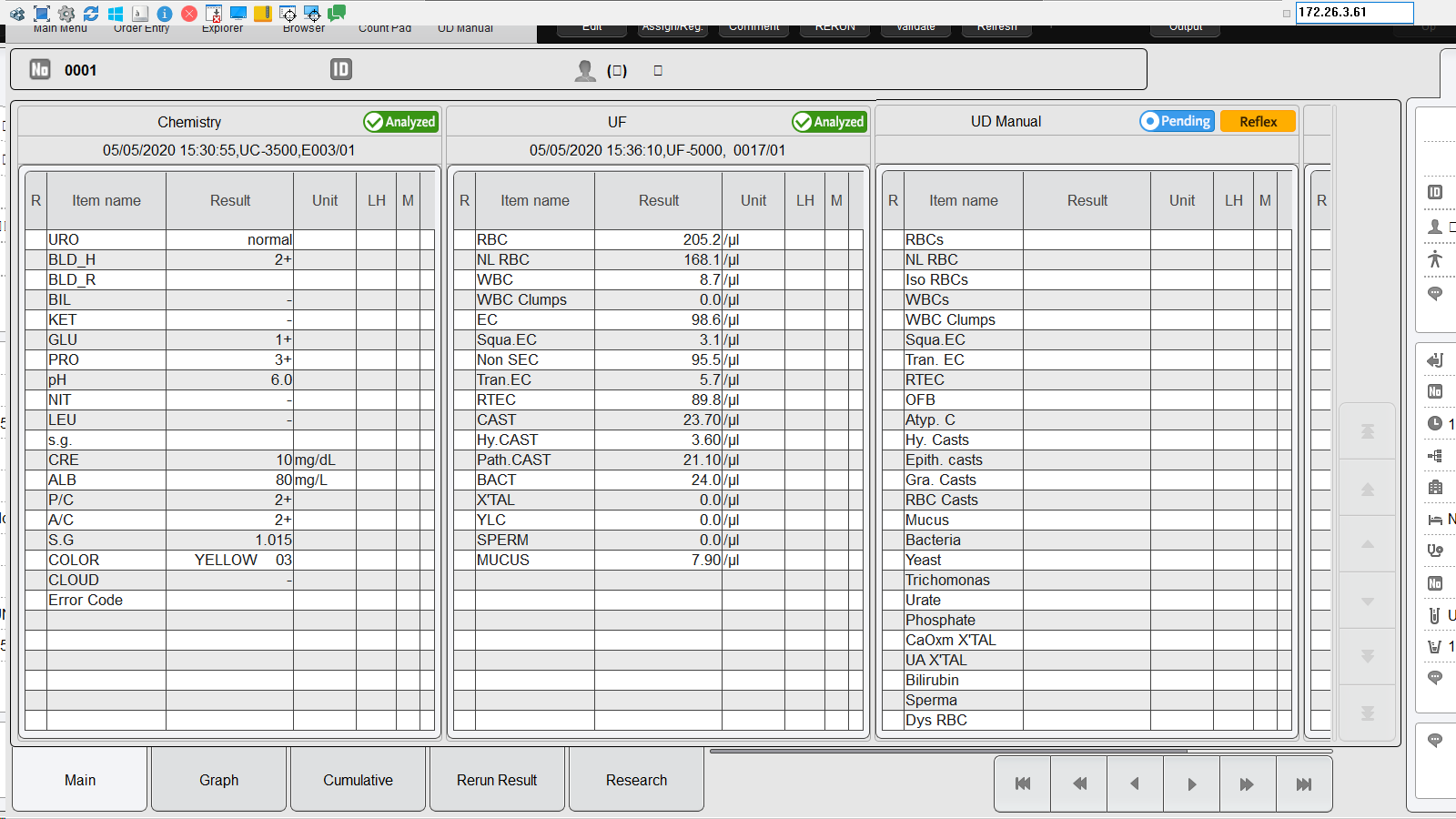
1. Urinalysis result display on the U-WAM
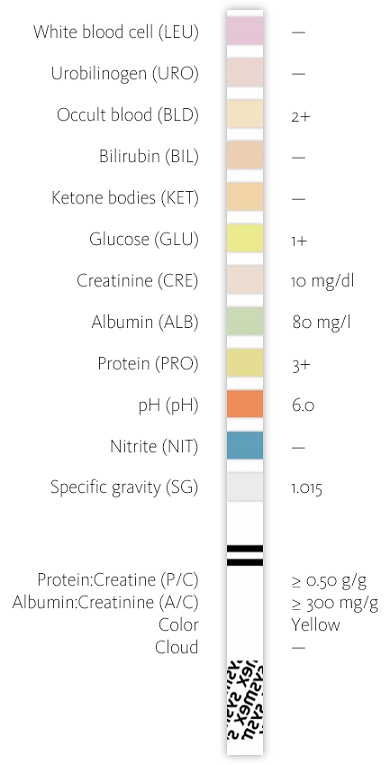
2. Dipstick testing on the UC-3500
Dipstick testing showed strong proteinuria and moderately increased albuminuria (formerly known as ‘microalbuminuria’). Since the urinary protein and albumin concentration can be affected due to excessive sweating or liquid uptake, correlation with the creatinine value is a common procedure to obtain accurate diagnostic information. Here, both the Protein:Creatinine ratio and the Albumin:Creatinine ratio confirmed severely increased albuminuria and proteinuria.
The use of Meditape 11A test strips on the UC-3500 and its CMOS sensor technology demonstrates the potential for highly sensitive detection and quantification of albuminuria with a dye-binding-based albumin test field. Albumin concentrations cannot only be graded but quantified with a limit of detection of 5.5 mg/L. Not only does it allow the determination of albuminuria in ranges of moderately increased albuminuria, but also in physiological ranges, comparable to immunonephelometric analysis [DELANGHE].
3. Renal tubular epithelial cells (RTEC) on the UF-5000
The UF-5000 detected renal tubular epithelial cells (RTEC). RTEC cover the renal tubules from the proximal tubule via the loop of Henle to the distal tubule and play a vital role in renal regeneration, but also release proinflammatory molecules that promote the progression of chronic kidney disease. Although a few RTEC may be present in the urine of healthy individuals due to normal exfoliation, the presence of ≥ 15 RTEC (per ten HPFs) indicates an active renal disease or tubular injury.
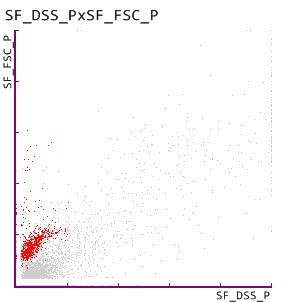
4. Dysmorphic RBC on the UF-5000
The UF-5000 further confirmed haematuria indicated by the UC-3500 by detecting dysmorphic RBC, which are known indicators of glomerular damage [Fairly and Birch].
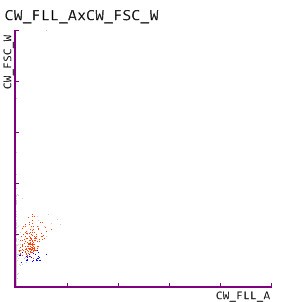
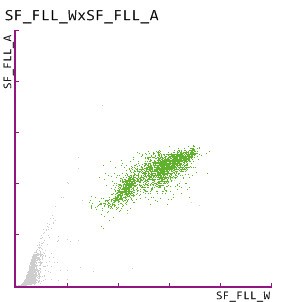
5. Urinary casts on the UF-5000 and the UD-10
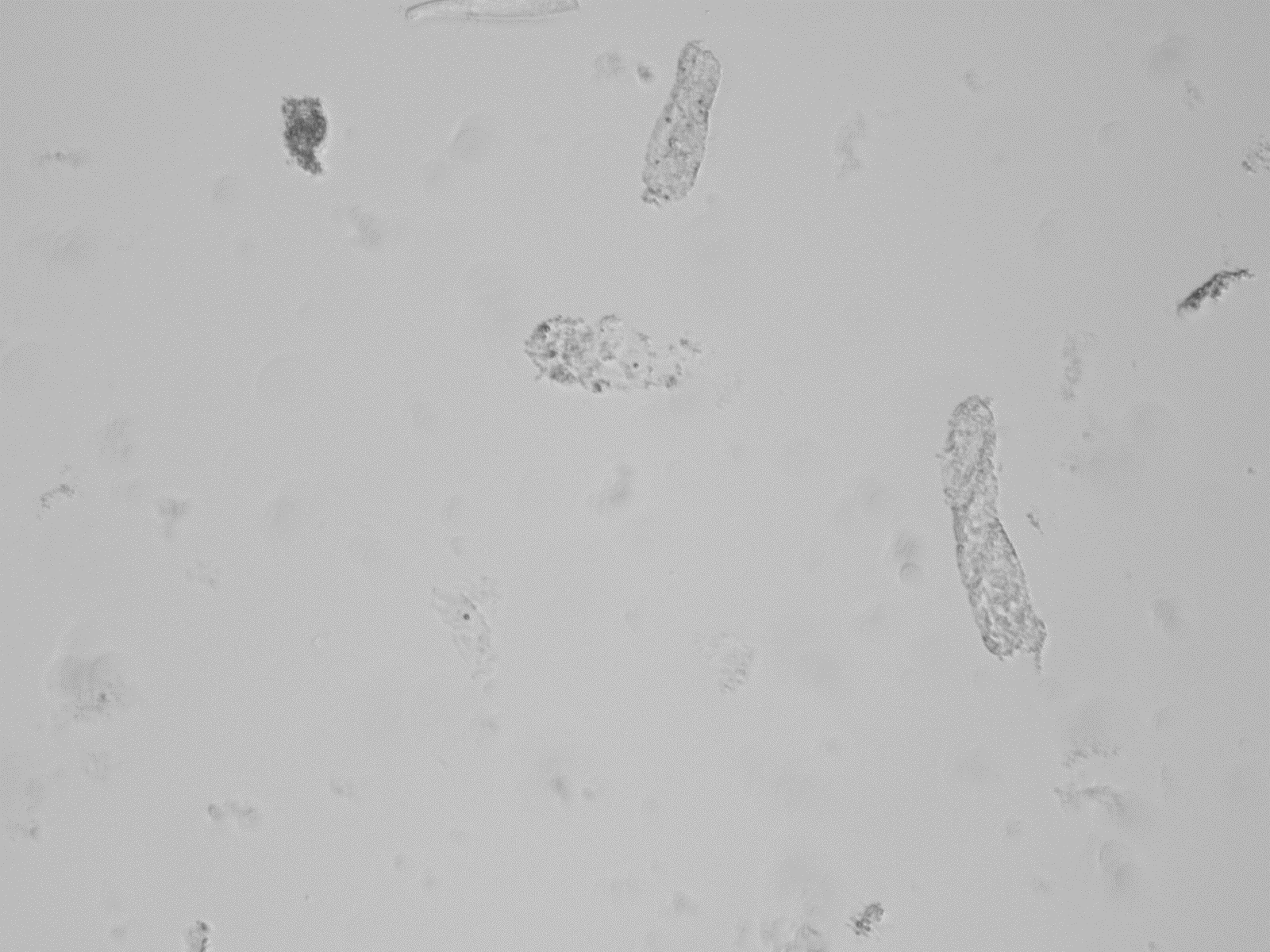
6. UD-10 image of pathological casts
The glycoprotein uromodulin, also known as Tamm-Horsefall protein, is exclusively synthesized by renal tubular cells in the distal loop of Henle [BACHMANN]. The precipitation and aggregation of uromodulin within the renal tubules leads to the formation of urinary casts. Hyaline casts are often observed in healthy individuals, but numbers increase with ongoing renal disease. Pathological casts as indicated in the above scattergram point out a renal disease, and their presence was confirmed by the detection of pathological casts by the UD-10.
References
Bachmann S, Koeppen-Hagemann I, Kriz W (1985): Ultrastructural localization of Tamm-Horsefall glycoprotein (THP) in rat kidney as revealed by protein A-gold immunocytochemistry. Histochemistry 83(6):531–538.
Cassia MA, Pozzi FE, Bascapè S, Saggiante L, Daminelli G, Cirelli C, Damavandi PT, Elli M, Gallieni M (2016): Proteinuria and albuminuria at point of care. Point of Care 2(1):e8–e16.
Delanghe JR, Himpe J, De Cock N, Delanghe S, De Herde K, Stove V, Speeckaert MM (2017): Sensitive albuminuria analysis using dye-binding based test strip. Clin Chim Acta 471:107–112.
Enko D, Stelzer I, Boeckl M, Derler B, Schnedl WJ, Anderssohn P, Meinitzer A and Herrmann M (2020): Comparison of the diagnostic performance of two automated urine sediment analysers with manual phase-contrast microscopy. Clin Chem Lab Med 58(2):268–273.
Fairley JK, Owen JE, Birch DF (1983): Protein composition of urinary casts from healthy subjects and patients with glomerulonephritis. Br Med J 287(6408):1838–1840.
KDIGO (2012): Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney inter., Suppl. 2013; 3:1–150.
Oyaert M, Delanghe JR (2019): Semiquantitative, Fully Automated Urine Test Strip Analysis. J Clin Lab Anal 33(5):e22870.
Pugh D, Gallacher PJ, Dhaun N (2019): Management of Hypertension in Chronic Kidney Disease. Drugs 79:365–379.
Seccia TM, Caroccia B, Calo LA (2017): Hypertensive nephropathy. Moving from classic to emerging pathogenetic mechanisms. Journal of Hypertension 35:205–212.
